

Background:
Factors determining inherent susceptibility to infection with the novel severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and the risk of severe outcomes in infected individuals remain poorly understood. Landsteiner ABO blood groups have been linked to host susceptibility to various infections through the interaction of the carbohydrate moieties defining ABO antigens with micro-organisms and the immune system. Previous studies of the original SARS coronavirus (SARS-CoV-1) demonstrated a decreased susceptibility to infection in group O individuals (Cheng et al. JAMA 2005; 293:1450-1) and the ability of plasma-derived anti-A antibodies to block the interaction between viral spike protein and human angiotensin-converting enzyme 2 receptor in vitro (Guillon et al. Glycobiology 2008; 18:1085-93). A recent genome-wide association study of patients with respiratory failure complicating coronavirus disease 2019 (COVID-19) suggested a higher risk of severe disease in group A, and a protective effect in group O (Ellinghaus et al. NEJM 2020 DOI:10.1056/NEJMoa2020283). Since the inception of the COVID-19 pandemic, a broad testing strategy was implemented in Kuwait and all individuals testing positive for SARS-CoV-2 were admitted to a single facility, including asymptomatic individuals. Here we examined the clinical outcomes of this cohort with respect to ABO blood group and compared its blood group distribution to that of the general population.
Methods:
All patients testing positive for SARS-CoV-2 by polymerase chain reaction assay of a nasopharyngeal swab specimen that were admitted to Jaber Hospital between February 24th to May 27th 2020 were included in the study. Relevant demographic and clinical data were extracted from hospital records. An anonymized summary of the distribution of blood types of the entire population of Kuwait was obtained from a national database and used as a control group. Clinical outcomes were in accordance with international consensus definitions. Appropriate statistical tests were used for bivariate analysis. Multivariate logistic regression was performed to determine relationships between variables of interest and outcome.
Results:
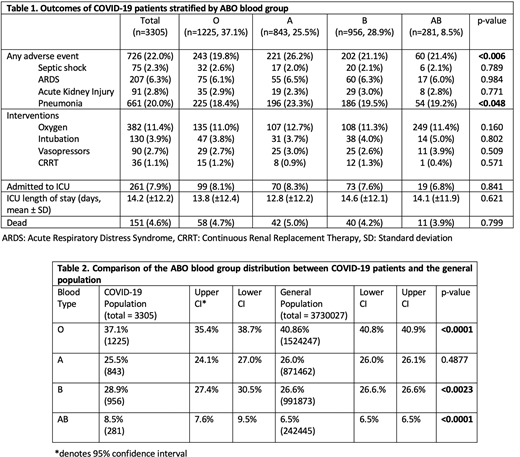
Of 3305 SARS-CoV-2 positive patients 37.1%, 25.5%, 28.9% and 8.5% were group O, A, B and AB respectively. 69.2% were male and 30.8% were female. Median age was 42 years. 48.1% were Kuwaiti citizens and 51.9% were non-Kuwaiti. Commonest comorbidities were hypertension (21.5%) and diabetes (20.1%). 17.4% were obese. 37.2% were asymptomatic on admission. There was no significant difference in baseline characteristics among the blood groups. Univariate analysis of clinical outcomes revealed no significant differences in need for oxygen support, admission to intensive care, intubation or death among the blood groups. However, rates of any adverse event and pneumonia differed significantly (Table 1). Multivariable analysis adjusted for age, sex, obesity and comorbidities showed that group A had higher odds of developing pneumonia compared to the other blood groups combined (adjusted odds ratio 1.32, 95% confidence interval 1.02-1.72, p<0.0363). We found no relationship between pneumonia and other blood groups. Compared to the general population, the COVID-19 cohort had a lower frequency of group O, equivalent frequency of group A and higher frequency of groups B and AB (Table 2). This trend was independent of nationality (Kuwaiti versus non-Kuwaiti). Incorporation of Rh (D) status did not impact the trend observed with ABO blood groups. Finally, no significant difference in Rh (D) status was found between the COVID-19 and general populations (Rh positive 93.4% versus 93.6% respectively, p=0.99)
Conclusion:
In a large, unselected patient population, no association between blood group and severe clinical outcomes in COVID-19 was found. Consistent with reports in other populations, we found a lower prevalence of blood group O in SARS-CoV-2 positive individuals and higher prevalence of blood group B and AB implicating a potential role of ABO blood group in susceptibility to infection. No association between SARS-CoV-2 infection with blood group A or Rh (D) group was found. Further examination of the mechanistic link between ABO antigens, antibodies and SARS-CoV-2, and its implications on controlling the current pandemic is warranted.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal